
Hysterectomy
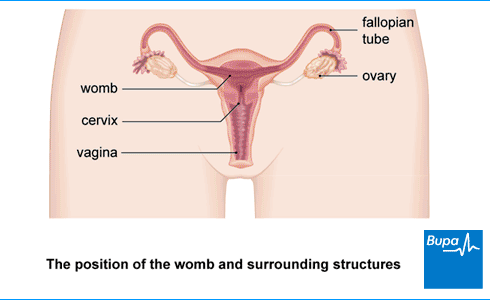
A hysterectomy is an operation to remove your womb (uterus). It can be a treatment option for several different medical conditions. After a hysterectomy, you’ll no longer have periods and you won’t be able to get pregnant.
About hysterectomy
You might have a hysterectomy operation for the following health conditions.
- Painful, frequent, or heavy periods.
- Fibroids – non-cancerous growths of muscle and fibrous tissue in your womb.
- Endometriosis – when the cells that usually line your womb also grow outside it.
- Adenomyosis – when cells that usually line your womb grow into the womb muscle instead.
- Prolapse of your womb – when your womb has dropped down from its normal position.
- If you have womb cancer, cervical cancer or ovarian cancer, vaginal cancer, or fallopian tube cancer.
For most of these conditions, you’ll usually try other treatments first. But if they don't work, or if your symptoms are severe, your GP may refer you to a gynaecologist for further investigation and treatment. A gynaecologist is a doctor who specialises in women’s reproductive health.
Your gynaecologist will talk to you about your treatment options, including any possible alternatives and the benefits and risks of having a hysterectomy. They’ll explain exactly what will happen before, during, and after the procedure.
Take your time before you make a decision whether to have a hysterectomy. It can sometimes be a major operation, depending on your circumstances. While some people find an end to their symptoms following a hysterectomy a huge relief, others struggle coming to terms with having their womb removed. Be sure to ask your doctor if you have any questions.
Types of hysterectomy surgery
There are three main ways to do a hysterectomy operation.
- Abdominal hysterectomy. Your surgeon will make a cut in your tummy (abdomen) to reach your womb.
- Vaginal hysterectomy. Your surgeon will carry out the operation through your vagina.
- Laparoscopic hysterectomy (keyhole surgery). Your surgeon will use a camera and instruments that they’ll insert through small cuts in your tummy.
There are also different types of hysterectomy.
- In a total hysterectomy, both your womb and cervix are removed.
- In a subtotal hysterectomy your womb is removed but your cervix is left in place.
- A radical hysterectomy involves removing surrounding tissues in addition to your womb and cervix.
- An oophorectomy or salpingo-oophorectomy involves removing one or both ovaries and fallopian tubes. You may have this at the same time as your hysterectomy.
Whichever type you have, you won’t have periods and you’ll no longer be able to get pregnant after a hysterectomy.
The type of hysterectomy you’re offered and how it’s done will depend on a number of things. These include why you’re having it, how severe the problem is, and whether you have any other health conditions. Talk to your doctor about your options, and what would be best for your particular circumstances.
Menopause after hysterectomy
If you have your ovaries removed as well as your womb, you’ll go through the menopause straight after the operation. This is called a surgical menopause. If you have a hysterectomy without having your ovaries removed, you may still go through the menopause earlier than usual.
You may decide to take hormone replacement therapy (HRT) to manage some of the symptoms of menopause. Normally, people take both oestrogen and progesterone (progesterone protects the womb). Since your womb is removed in a hysterectomy, you won’t need to take progesterone, only oestrogen. Your doctor will talk to you about the menopause and the treatments available to help with symptoms.
Cervical screening after hysterectomy
If your cervix is removed as part of your hysterectomy, you’ll no longer need cervical screening (‘smear’) tests after the operation. If you have a hysterectomy that leaves your cervix in place, you should carry on having cervical screening tests.
Preparing for a hysterectomy
Before the operation
Your doctor will give you information about how to prepare for your hysterectomy operation. For example, if you smoke, they’ll ask you to stop. Smoking increases your risk of complications during and after your surgery. It can also slow your recovery.
You may need to have some tests, such as blood tests and an electrocardiogram (ECG) before your operation. This is to make sure that you’re well enough for the operation to go ahead as planned.
How long you need to stay in hospital depends on what type of hysterectomy you have, and how the operation is done. It may be a day or two after vaginal or laparoscopic surgery, but it may be longer if you’re having a hysterectomy to remove cancer. Your surgeon will advise you before the procedure. Make sure you arrange for someone to drive you home after your operation.
On the day
You’ll usually need to stop eating and drinking around six hours before your hysterectomy operation. You may be able to continue drinking water up to two hours beforehand. Follow any instructions your hospital gives you.
At the hospital, you’ll be asked to wear compression stockings to help prevent blood clots forming in the veins in your legs. You may have an injection of an anti-clotting medicine too.
You’ll meet your surgeon before the procedure. They’ll check if you’re happy to go ahead and ask you to sign a consent form.
Hysterectomy procedure
If you’re having an abdominal or a laparoscopic hysterectomy, you’ll usually have it under general anaesthesia. This means you’ll be asleep during the operation. For a vaginal hysterectomy, you’ll have a spinal anaesthetic, epidural, or a general anaesthetic. With a spinal anaesthetic or epidural, you’ll be awake but you’ll feel no pain from the waist down.
Abdominal hysterectomy
If you have an abdominal hysterectomy, your surgeon will make a cut across your lower tummy (abdomen). The cut may be along your bikini line. Sometimes your surgeon will make the cut from your belly button down to your bikini line instead. Your surgeon will then remove your womb and any other parts – such as your cervix, ovaries, and fallopian tubes – through the cut.
At the end of the operation, they’ll close your wound with stitches or clips.
Vaginal hysterectomy
In this method, your surgeon will insert instruments into your vagina to do the operation. They’ll make a cut around the lower part of your womb to take out your cervix and womb. They’ll then attach your vagina to ligaments in your pelvis using stitches.
Laparoscopic hysterectomy
Laparoscopy is sometimes called ‘keyhole surgery’. In this procedure, your surgeon will make three small cuts in your lower tummy. They’ll gently inflate your abdomen using carbon dioxide gas. This will allow your surgeon to see inside your tummy more clearly. Your surgeon will then insert surgical instruments with a tiny camera to remove your womb and cervix. Or they’ll use robotic instruments that they’ll control at a nearby console.
Aftercare for hysterectomy
In hospital
You’ll be in a recovery room once you wake up after your hysterectomy operation. You’ll need to rest until the effects of your anaesthetic have worn off. You’ll usually feel sleepy after a general anaesthetic and you might find it difficult to think clearly. This should pass within 24 hours. You might have some discomfort as the anaesthetic wears off but you'll be offered pain relief.
You’ll have a catheter in overnight after your hysterectomy operation. This drains urine through a tube and into a bag. Your nurse will remove it the next day, once you’re able to get up out of bed and move around. You may also have a drip to give you fluids and pain medication. After a vaginal hysterectomy, you may have a gauze pack inside your vagina to control bleeding for the first 24 hours. A nurse will remove this before you go home.
You’ll be able to start eating and drinking as soon as you feel ready. Eating and drinking can help you get back to normal and feel ready to go home.
Going home
Your healthcare team will monitor you and tell you when you can go home. This might be within the first 24 hours for a vaginal or laparoscopic hysterectomy, but it can be after two or three days. It’s likely to be between three and five days following an abdominal hysterectomy.
You won’t be able to drive straightaway, so you’ll need someone to take you home.
Caring for your wounds
Before you go home, your nurse will advise you about caring for your wounds and may arrange a date for a follow-up appointment.
You should be able to have a shower or bath and remove any dressings the day after your operation. Pat your healing wounds to dry them.
If you’ve had a vaginal hysterectomy, you won’t have any wounds on the outside of your body. Stitches inside your vagina will be dissolvable, but you may notice them come out on their own after a few days or weeks. This is normal. They should completely dissolve after five to six weeks.
Often, any stitches you have will dissolve on their own and you won’t need to have them removed. But sometimes with an abdominal or laparoscopic hysterectomy, you may have stitches or staples that need to be removed. This can usually be done by the practice nurse at your GP surgery around five to seven days after your operation.
Recovery from hysterectomy
It usually takes a few weeks to recover from a hysterectomy operation but this is different for everyone. It may take longer. Although you need to rest, it will help with your recovery to start doing some gentle exercise and get back to your normal activities. Build up your activity slowly and gradually. Don’t lift anything heavy or do any strenuous activity for at least three to four weeks after having a hysterectomy.
Having sex
You can have sex six weeks (or more) after your hysterectomy operation, once all your wounds (inside and out) heal. You won’t need to use contraception to prevent pregnancy after a hysterectomy. But you will still need to use condoms to protect against sexually transmitted infections (STIs).
Pelvic floor exercises
It’s important to do pelvic floor exercises as part of your recovery, to strengthen these muscles. Your pelvic floor muscles help to hold your abdominal organs in the right place and keep your bladder and bowel closed. You may see a physiotherapist before you’re discharged from hospital, who will show you how to do these. Or ask your surgeon when you can start to do pelvic floor exercises.
Going back to work
When you go back to work will depend on the type of job you do, how physical it is and how well you feel. It might be two to three weeks after surgery if you’re feeling well and there are no complications from your surgery. But it can take longer for some people, especially if your job is more physical. You’ll usually recover faster following a vaginal or laparoscopic hysterectomy than an abdominal hysterectomy.
Driving
If you’ve had a vaginal or laparoscopic hysterectomy, it can take two to four weeks before you feel comfortable and safe enough to drive. If you’ve had an abdominal hysterectomy, this may take longer. Check with your motor insurance provider in case they have specific conditions for driving after surgery.
Side-effects of a hysterectomy
Hysterectomy side-effects can include the following.
- Pain and discomfort in your lower abdomen for some weeks after your operation but it should improve as you recover. Your nurse will provide you with some painkillers to manage this.
- Pain in your shoulder following a laparoscopic hysterectomy. It’s caused by the gas used to inflate your tummy irritating a nerve. You can take painkillers to manage this.
- Trapped wind. This is caused by your bowel temporarily slowing down, and it can feel uncomfortable. Walk around as much as you can as it will help.
- Light bleeding or spotting from your vagina for up to six weeks after your operation. Wear a sanitary pad, rather than using a tampon, until any bleeding stops.
Complications of a hysterectomy
Complications are problems that can occur during or after the operation. Some of the possible complications after a hysterectomy are as follows.
- Heavy bleeding (more than would normally be expected after hysterectomy). This is more common after abdominal hysterectomy.
- Infection of your wound. The skin around your scars may become very red and sore.
- Vaginal infection following vaginal hysterectomy. You may have a fever, foul-smelling discharge from your vagina and pain in your pelvis.
- A urine infection. You may need to pee urgently and more often, have pain, or discomfort when you’re peeing and smelly or cloudy pee.
- Damage to blood vessels or organs in your abdomen, including your bowel, bladder, or tubes that lead from your kidneys to your bladder (ureters). It can cause loss of sensation in your bladder, needing to pee more often, and constipation. If you have severe or worsening pain, vomiting, and a fever, seek medical attention.
- Deep vein thrombosis (DVT) – a blood clot in a vein in your lower leg. This may cause your leg to become red, swollen, and painful. It can be dangerous if it travels to your lungs (pulmonary embolism).
Contact the hospital where you had your hysterectomy if you develop any problems. You should seek urgent medical attention if you have severe pain, or signs of an infection, or DVT.
Sepsis (adults)
Sepsis is an extremely rare life-threatening complication of hysterectomy that can develop if you get an infection. Sepsis is a medical emergency. Call 999 or go to A&E immediately if you have any of the following symptoms.
- Slurred speech, confusion, difficulty making sense.
- Extreme shivering or muscle pain.
- Passing no pee (urine) during a day.
- Severe difficulty breathing, feeling breathless, or breathing very fast.
- It feels like you’re going to die.
- Skin changes, such as your skin looking blue, pale, or blotchy, or a rash that does not fade when you roll a glass over it.
Alternatives to hysterectomy
Depending on why you have been offered hysterectomy, there may be alternative treatments you can try. For conditions like fibroids and endometriosis, your doctor will usually suggest medicines or hormone treatments first. You’ll usually only be offered surgery if these treatments haven’t worked. Other surgical procedures may include:
- Myomectomy. This is surgery to remove fibroids. It doesn’t remove your womb, so it won’t affect your ability to get pregnant.
- Endometrial ablation. This is a procedure to treat heavy periods. It destroys the lining of your womb, but avoids a major operation like hysterectomy to remove your womb.
- Uterine artery embolisation. This is a procedure to treat fibroids. It involves an injection to cut off the blood supply to the fibroids. This destroys them or stops them growing.
- Levonorgestrel intrauterine devices (LNG-IUDs). Also known as a coil, it’s an alternative to hysterectomy to manage heavy periods.
If you have cancer of your womb, hysterectomy is usually the only possible option to cure the cancer.
Whatever your situation, talk to your doctor about the treatment choices available to you.
Worried about your gynaecological health?
Get a picture of your current health and potential future health risks with one of our health assessments.
To book or to make an enquiry, call us on 0370 218 8122
For most people, it takes around three to five weeks to recover from a hysterectomy. It can be different for everyone, and will depend on the type of operation you have, and your general health.
Yes, you should be able to have a normal life after a hysterectomy but it depends on your individual circumstances and why you needed it. One change to be aware of is if you have your ovaries removed as well as your womb, you will go through the menopause straight after the operation. Your doctor will talk to you about this and the treatments available to help with menopause symptoms.
See our Types of hysterectomy surgery section for more information.
You’ll have a hysterectomy under a general anaesthetic, spinal anaesthetic, or epidural so you won’t feel any pain during the procedure. You might have some discomfort as the anaesthetic wears off but you'll be offered pain relief. Pain and discomfort in your lower abdomen is likely for a few days after your operation. Your nurse will provide you with some painkillers to manage this.
A hysterectomy isn’t usually major surgery because most operations don’t involve open surgery (see the treatment section), which usually means a short stay in hospital and quick recovery. But it can greatly impact your quality of life and have long-term physical, psychological, and mental health effects. So it’s important to discuss the operation with your doctor to understand the benefits and risks.
Menopause
Hormone replacement therapy (HRT)
Endometriosis
Fibroids
Did our Hysterectomy information help you?
We’d love to hear what you think. Our short survey takes just a few minutes to complete and helps us to keep improving our health information.
The health information on this page is intended for informational purposes only. We do not endorse any commercial products, or include Bupa's fees for treatments and/or services. For more information about prices visit: www.bupa.co.uk/health/payg
This information was published by Bupa's Health Content Team and is based on reputable sources of medical evidence. It has been reviewed by appropriate medical or clinical professionals and deemed accurate on the date of review. Photos are only for illustrative purposes and do not reflect every presentation of a condition.
Any information about a treatment or procedure is generic, and does not necessarily describe that treatment or procedure as delivered by Bupa or its associated providers.
The information contained on this page and in any third party websites referred to on this page is not intended nor implied to be a substitute for professional medical advice nor is it intended to be for medical diagnosis or treatment. Third party websites are not owned or controlled by Bupa and any individual may be able to access and post messages on them. Bupa is not responsible for the content or availability of these third party websites. We do not accept advertising on this page.
- Hysterectomy. Medscape. emedicine.medscape.com, updated 16 October 2024
- Hysterectomy. FAQs. American College of Obstetricians and Gynecologists. acog.org, last updated September 2024
- Menorrhagia. Patient. patient.info, last updated 13 August 2024
- Fibroids. NICE Clinical Knowledge Summaries. cks.nice.org.uk, last revised April 2023
- Endometriosis. Patient. patient.info, last updated 24 June 2024
- Gunther R, Walker C. Adenomyosis. StatPearls Publishing. ncbi.nlm.nih.gov/books, last updated 12 June 2023
- Genitourinary prolapse. Patient. patient.info, last updated 19 January 2022
- Carugno J, Fatehi M. Abdominal hysterectomy. StatPearls Publishing. ncbi.nlm.nih.gov/books, last updated 18 July 2023
- Perioperative care in adults. National Institute for Health and Care Excellence (NICE). nice.org.uk, published 19 August 2020
- Pillarisetty LS, Mahdy H. Vaginal hysterectomy. StatPearls Publishing. ncbi.nlm.nih.gov/books, last updated 24 April 2023
- Radical hysterectomy. Medscape. emedicine.medscape.com, updated 13 May 2022
- Having a hysterectomy. Endometriosis UK. endometriosis-uk.org, last updated October 2022
- Guidance. Ceasing and deferring women from the NHS cervical screening programme. NHS England. gov.uk, updated 27 September 2024
- Smoking and surgery. Action on Smoking and Health. ash.org.uk, published April 2023
- Before your operation for cervical cancer. Cancer Research UK. cancerresearchuk.org, last reviewed 27 October 2023
- Surgery to remove the womb (radical hysterectomy). Cancer Research UK. cancerresearchuk.org, last reviewed 27 October 2023
- After cervical cancer surgery. Cancer Research UK. cancerresearchuk.org, last reviewed 30 October 2023
- Vaginal hysterectomy – recovering well. Royal College of Obstetricians and Gynaecologists. rcog.org.uk, accessed 14 January 2025
- Venous thromboembolism in over 16s: Reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism. National Institute for Health and Care Excellence (NICE). nice.org.uk, last updated 13 August 2019
- Hysterectomy. British Fibroid Trust. britishfibroidtrust.org.uk, last updated 1 February 2021
- Zhao Y, Xin W, Luo X. Post-laparoscopic shoulder pain management: A narrative review. Curr Pain Headache Rep 2025; 29(18). doi: https://doi.org/10.1007/s11916-024-01355-y
- Problems after cervical cancer surgery. Cancer Research UK. cancerresearchuk.org, last reviewed 1 November 2023
- Vaginitis. Medscape. emedicine.medscape.com, updated 25 March 2024
- Urinary tract infection (lower) – women. NICE Clinical Knowledge Summaries. cks.nice.org.uk, last revised December 2024
- Sepsis. Patient. patient.info, last updated 21 February 2024
- Sepsis in adults. BMJ Best Practice. bestpractice.bmj.com, last reviewed 22 December 2024
- Gynecologic myomectomy. Medscape. emedicine.medscape.com, updated 16 July 2021
- Menorrhagia (heavy menstrual bleeding). NICE Clinical Knowledge Summaries. cks.nice.org.uk, last revised November 2024
- Endometrial cancer. BMJ Best Practice. bestpractice.bmj.com, last reviewed 22 December 2024