
Endometriosis
Endometriosis is when cells similar to those in the lining of your womb (uterus) appear in other parts of your body, most commonly in your pelvis. When you have a period, these cells can build up and break away in the same way as your womb lining. This causes painful inflammation in surrounding tissues.
About endometriosis
About one in every 10 people assigned female at birth and of child-bearing age has endometriosis. But it could affect as many as half of people who have infertility. Endometriosis usually stops causing symptoms after the menopause.
Before your period, your womb lining thickens to receive a fertilised egg. If you don’t get pregnant, the lining of your womb breaks down and leaves your body as menstrual blood (a period) each month. This process is controlled by your body’s hormones.
In endometriosis, cells like those that line your womb (endometrial tissue) are also elsewhere in your body. This tissue thickens, breaks down and bleeds with your menstrual cycle. As your body tries to get rid of this endometriosis tissue, the process causes scarring and irritation, and results in pain.
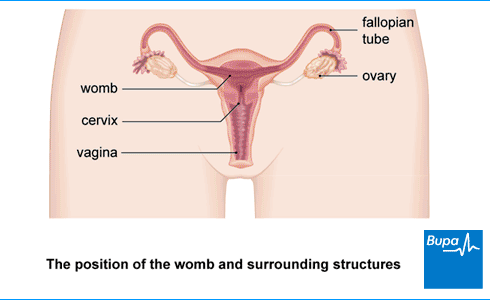
Endometriosis usually affects tissues inside your pelvis. It’s most commonly found in and around your ovaries and fallopian tubes, and the surrounding ligaments. It is also frequently found between your womb and the end part of your bowel (rectum). If you have endometriosis on your fallopian tubes or ovaries, it can lead to fertility problems.
Endometriosis can affect other parts of your body, such as your lungs, but this is rare.
Endometriosis isn’t a type of cancer, and you can’t catch it or give it to anyone else.
Causes of endometriosis
Doctors don’t yet know exactly what causes endometriosis. There are different ideas about how it develops but none of these fully explain why endometriosis happens. It’s probably caused by a combination of things. For example, your immune system or hormones might play a role. Endometriosis may also run in families – you’re more likely to get it if your mother or sister has it.
Some things may increase your risk of getting endometriosis. These include if you:
- started your periods early
- haven’t given birth to any children
- have a low body mass index (BMI)
- have an autoimmune disease (a condition caused by your immune system attacking healthy body tissues)
- smoke
Symptoms of endometriosis
One of the most common endometriosis symptoms is pain in your pelvis, which is usually worse just before and during your period. Endometriosis pain may get worse over time and you may find that it doesn’t get better when you take over-the-counter painkillers such as ibuprofen.
Other endometriosis symptoms include:
- pain during or after sex
- heavy periods
- feeling extremely tired (fatigue)
- difficulty getting pregnant (conceiving)
You may become depressed or anxious because of the long-term pain.
Less common endometriosis symptoms include the following.
- Endometriosis on your bowel can cause pain when you poo (have a bowel movement). You may have blood in your poo during your period.
- If you have endometriosis on your bladder, it can be painful when you pee (pass urine). You may see blood in your pee.
These symptoms can also be caused by conditions other than endometriosis. If you have any of them, see a GP.
Endometriosis symptoms often ease during pregnancy, and they may stop without any treatment.
You might not have any endometriosis symptoms, and only find out that you have endometriosis after tests for something else – for example, infertility.
Do you need help with managing your endometriosis symptoms?
Our Period Plan offers fast access to women's health experts to support conditions like endometriosis.
Diagnosis of endometriosis
Your GP will ask about your symptoms to help make an endometriosis diagnosis. Don’t be embarrassed to tell them about the problems you’re having – including pain during sex or seeing blood when you go to the toilet. It’s important that they know everything.
Your GP may offer you the following tests or refer you to a gynaecologist (a doctor who specialises in women’s reproductive health) for the tests.
Vaginal examination
In a vaginal examination, your doctor will put on some gloves, add some lubricant then insert their fingers into your vagina. They’ll use their other hand to press lightly on your tummy (abdomen) and will gently feel for any abnormalities in and around your womb.
This examination may feel uncomfortable but shouldn’t be painful. Let your doctor know if anything hurts. You can ask to have someone with you while you have this test, if you prefer not to be alone.
Scans
You may have an ultrasound scan, in which a probe will be put into your vagina. This can help to pick up endometriosis or other causes of your symptoms. But there’s a chance that it won’t pick up endometriosis, even if you have it.
You might also be offered a magnetic resonance imaging (MRI) scan. This can help to diagnose endometriosis that’s deep inside your pelvis or that affects your bladder or bowel.
Laparoscopy
It can take time diagnosing endometriosis because the symptoms are similar to other health conditions. The only way doctors can be sure is to check with a procedure called a laparoscopy. You have this under general anaesthetic so you’ll be asleep. Your gynaecologist will look inside your tummy (abdomen) with a laparoscope. This is a narrow tube with an eyepiece that they will put into your tummy through a small cut. They may take a small sample of tissue (biopsy) to send to the lab for examination under a microscope.
If you have a laparoscopy to diagnose endometriosis, your gynaecologist may destroy or remove the endometriosis at the same time. Or they may recommend you have surgery to remove it later. For more information, see our section on treatment.
Sometimes, rather than having this procedure right away, your doctor may suggest you try other treatments first. For example, they might suggest hormonal medicines, to see if they help.
Treatment of endometriosis
Treatment for endometriosis symptoms will depend on how bad your symptoms are, and if you want to have children in the future. Your doctor will discuss the various options with you, and help you decide which endometriosis treatment is best for you.
Pain medicines
Your doctor will probably suggest that you try a non-steroidal anti-inflammatory medicine (NSAID), such as ibuprofen to ease pain and discomfort. Paracetamol is an alternative that you can take alone or with an NSAID. You can buy these pain medicines over the counter from a pharmacy.
If these medicines don’t help, your doctor might prescribe a different medicine for pain.
Always read the patient information leaflet that comes with your medicine. If you have any questions, ask a pharmacist for advice.
Hormone treatments
Hormone treatments can help to reduce areas of endometriosis tissue and so lessen your pain. They aren’t suitable to treat endometriosis if you’re trying to get pregnant because they’re contraceptives. But they won’t have any effect on having children in the future.
Your doctor may offer you the combined oral contraceptive pill. This may be for around six months at first, but if it’s helpful, you can usually continue to take it. If that doesn’t help, or doesn’t suit you, there are two other types of hormonal treatment that your doctor may offer.
- Progestogens. You can take these as tablets, as an injection every three months or in an intrauterine system (coil)
- Gonadotrophin-releasing hormone (GnRH) agonists. You can have these as injections, an implant, or a nasal spray.
Each of these treatments has its own side-effects. Your doctor can explain these and discuss which treatment will suit you best.
Surgery
It’s possible to have areas of endometriosis treated or removed with surgery. If endometriosis affects your fertility, this can help to improve your chance of getting pregnant and can also reduce pain. You have endometriosis surgery under general anaesthesia so you’ll be asleep. Endometriosis can come back after surgery, so you may need to have surgery again in the future.
Laparoscopy (keyhole surgery)
You may have a laparoscopy – a type of keyhole surgery to treat endometriosis. Your gynaecologist will make a small cut and put in a narrow tube with an eyepiece (laparoscope) to look inside your tummy (abdomen). They may be able to see and remove or destroy patches of endometriosis.
Laparotomy (open surgery)
Rarely, if you have severe endometriosis, keyhole surgery may not be suitable. You may need an operation called a laparotomy where a surgeon will make a larger cut in your tummy (abdomen), usually along your bikini line. Your gynaecologist will explain the procedure and why it may be best for you.
Hysterectomy
If you don’t want to have children in the future, your gynaecologist may suggest a hysterectomy. This is a larger operation to remove your womb, and often also your ovaries. This operation can also be done using keyhole surgery.
If you have your ovaries removed, you’re likely to have menopause symptoms afterwards, such as hot flushes. Your specialist may suggest you take hormone replacement therapy (HRT). Talk to your gynaecologist about the pros and cons of this type of endometriosis surgery.
Complications of endometriosis
Complications of endometriosis include the following.
- Scar tissue can attach to organs in your pelvis and tummy (abdomen). These scars are known as adhesions. Adhesions are often already present when you have endometriosis and this can cause pain, but surgery can also increase your risk of getting adhesions.
- You may have difficulty getting pregnant (reduced fertility). This affects around a third of people with endometriosis
- Endometriosis can cause ovarian cysts (called endometriomas or chocolate cysts). These can rupture and cause pain and affect your fertility.
Endometriosis isn’t a cancer and doesn’t cause cancer. Statistically, there’s a slight increase in risk of ovarian cancer, breast cancer and thyroid cancer but the risk is very small.
Speak to a GP or doctor if you have any questions about the complications of endometriosis.
Endometriosis: your questions answered
Transcript
Who are you and what is your background?
Hello.
My name's Dr. Rebecca Rohrer.
I'm a doctor, practising clinically, a medical director at
Bupa, and I've got a passion for women's health.
What is endometriosis?
Endometriosis is a condition where the lining
that is normally inside the womb can grow outside it.
So in places like the fallopian tubes, the ovaries,
and even sometimes in the areas lining the pelvis
and in places like the bladder or bowel.
Who gets endometriosis?
Endometriosis affects about 10%
of reproductive age women around the world,
that's about 190 million women. In the UK,
about 1.5 million women are living with endometriosis.
What causes endometriosis?
The causes of endometriosis is still an area
of intense research
and there's lots of interest in it, given
how many women are affected by it. There are a few theories.
The first is that it may be associated with genetics,
endometriosis is known to run in families,
and we also know that certain
ethnic groups are affected more than others.
The second is that it may be to do with the immune system,
which is the body's ability to be able
to fight infections or foreign bodies.
And finally, there's a theory that the cells
that line the womb, called endometrial cells, could spread
around the body, either by the blood
or the lymphatic system.
And the lymphatic system is a series of tubes
and glands that helps the body fight infection.
What are the symptoms of endometriosis?
Endometriosis has lots of symptoms
and it's important to remember
that not all women will be affected equally.
Some women will have no symptoms, some will have lots
of symptoms, and it'll really affect their quality of life.
Many women do report heavy periods where they're having
to change their tampons or their pads really frequently
and painful periods,
and the pain can be so bad
that it stops them doing their day-to-day activities.
Women can also report that they get blood in their pee
or poo, and sometimes people can report lots
of low abdominal pain or pelvic pain,
and sometimes pain during or after sex.
There are other symptoms as well, like bloating,
changes in your bowel habit, so for diarrhoea
and constipation, and obviously all
of these symptoms can have a really big impact on women's
lives, and so low mood and depression can also be a symptom.
How is endometriosis diagnosed?
Endometriosis can be a real challenge to diagnose.
That's because there are lots of symptoms
and those symptoms can also be
because of lots of other diseases and conditions,
and in fact, there's good evidence that from first symptoms
to diagnosis can be as long as seven
and a half years, unfortunately.
Now, the first step should be speaking to your doctor
or GP so that they can get an understanding of
what symptoms you're having
and whether there's any pattern to them.
If the GP isn't able to make a diagnosis
or if some of the treatments
that they recommend aren't working particularly well,
they might refer you
to a specialist gynaecologist in a hospital.
Now, the gynaecologist may want to do some further tests.
They might include an ultrasound scan of the tummy
and the pelvis or an MRI scan
to look at that in more detail.
It's also an option that they may want to do a laparoscopy.
Now a laparoscopy is an operation where you're put to sleep
and a small camera is inserted
through a cut near your tummy button,
and that allows the gynaecologist to look inside the pelvis
for any signs of endometriosis.
I think I have endometriosis - what should I do?
There's good evidence out there that women with symptoms
of endometriosis often don't go and see a doctor about them,
and that's because they may feel
that the symptoms are a normal part of having a period
or that they're not serious enough to see a doctor. Actually,
because endometriosis can be such a difficult condition,
it's really important that you go
and see a doctor about them.
I'd really recommend keeping a diary of your symptoms
either in a notebook
or there are apps available, ideally over a couple of cycles
so that the doctor can get an idea
around whether these symptoms relate to your monthly cycle,
but if the symptoms are having a big impact on your quality
of life, it's really important to see a doctor as soon
as possible.
I think I have endometriosis but am not getting the support I need - what should I do?
It's really important for women
who feel like their symptoms may be caused by endometriosis
to firstly make a careful record of their symptoms,
ideally over a couple of cycles so that
any doctor seeing them can understand the impact
of their monthly cycle on those symptoms.
However, for women who feel
that the symptoms are having a major impact on their quality
of life, I'd really recommend going
to see your doctor or GP as soon as possible.
The doctor or GP can do a lot in terms
of initial treatment and investigations.
If they feel it's necessary, they may want to refer you
to a specialist gynaecologist in a hospital.
It's also really important to remember
that there's lots of support out there.
There's charities offering support groups nationwide,
helplines, and information available online, so women
with these symptoms really don't need to suffer alone.
Can endometriosis affect my fertility?
We know that unfortunately, women with endometriosis
can have issues with their fertility,
but that doesn't apply to all women with endometriosis.
Now, any issues are likely to be
because of damage to the ovaries or the fallopian tubes,
but this is still an area of intense research.
Now, women who want to try to conceive with endometriosis
or the symptoms of endometriosis should really go
to see their doctor or GP as soon as possible, and that's
because even though the treatments to treat the symptoms
of endometriosis don't impact
or improve the chances of fertility.
Actually, there are lots of other options.
That includes referral to fertility clinics to be able
to support some of your decisions and options,
but also referral to gynaecologists
and their options include operations that might be able
to remove some of the areas of endometriosis in the pelvis
that are causing damage.
Whilst none of this can guarantee a chance of pregnancy,
it's really important to be able
to support your fertility journey going forward.
Can endometriosis affect my periods?
We know that for some women with endometriosis,
their periods can be really affected.
Women can find that their periods are really painful.
That means that it's so painful that they're not able
to do their day-to-day activities,
even if they're taking pain relief.
Women can also find that their periods are really heavy.
That means that they're passing clots, they're using lots
of tampons or pads
and even bleeding through into their clothes,
which can obviously have a massive
impact on their quality of life.
Women can also get bleeding in between their periods,
so away from their usual cycle.
It's really important that for women with these symptoms,
they're keeping a record of:
how it's affecting them, when their symptoms are happening,
and how it relates to their normal cycle.
That's important because when they go
and speak to their doctor or GP,
it can give them an understanding of any patterns,
and it really helps the doctor or GP to make decisions about
what treatment to start
because there are lots of options in terms
of medication here.
Also, helps you to keep a record of
how the treatment's working for you
and whether you'd like to continue with it.
Does endometriosis run in families?
Endometriosis is known to run in families,
so there's some evidence that there may be a genetic element
to the condition. For women who feel
that their symptoms may be because of endometriosis,
it's therefore, really important to speak
to any close female relatives to understand whether
they may have similar symptoms
or whether they've ever been diagnosed with a condition.
I'd also really recommend that when you go
and speak to your GP or doctor,
you mention anybody else in the family who might be affected
by the condition.
Can you get endometriosis post-menopause?
We know that, very rarely, new symptoms
of endometriosis can develop up to 10 years
after the menopause.
This is really rare
and there are lots of other reasons
for why you might have changes in your periods
or bleeding patterns or pelvic pain at that age.
So it's really important that you speak to your doctor
or GP if you notice any of these symptoms.
Can children get endometriosis?
Endometriosis is a condition
that impacts the menstrual cycle. So, the symptoms
of it often only become apparent once menstrual cycles are
established, and that can take a couple of years
after periods start.
That means endometriosis is much more a condition affecting
teenagers upwards.
However, it can obviously take some time to get
to know your periods and what they're like,
and I'd say, if you
or your child is experiencing symptoms
that you feel are either not normal
or are really affecting their quality of life,
it's really important that you go and speak to your doctor
or GP as soon as possible.
What are the treatments for endometriosis?
There are lots of treatment options available
for endometriosis.
While these can't cure the condition,
they can really help women to improve the symptoms
and the impact of those on their quality of life.
Treatments broadly aim to reduce pain,
reduce the heaviness of women's periods, help
to improve fertility,
and to minimise the damage caused by endometriosis In terms
of removing tissue when it's outside the womb.
Treatment options vary massively based on a patient's
personal preference, the severity of their symptoms.
It can also vary by how bad the endometriosis is
and where it is. It may also depend on
when a woman wants to try and get pregnant, if at all,
and whether they want to use contraception. Broadly,
that means that there are lots of options available
to people, and that really underlines the importance
of understanding your symptoms, understanding
how they relate to your monthly cycle,
and thinking about what's important to you so
that when you go and speak to your doctor,
you can have a really honest conversation with them.
What are the side effects of different treatments?
There are so many treatments available for endometriosis.
It's really important to be aware that
with all medications, there can be side effects.
However, the side effects vary so much
between different treatments,
and some women won't have any side effects at all.
What I'd really recommend is that if your doctor
or GP recommends a new treatment for you,
you can have a conversation
with them about any potential side effects
and even ask for any online resources that you might be able
to read from them
that could give you a bit more information about
potential side effects.
What that's going to allow you to do is
to weigh up any potential benefits
of the treatment versus any side effects,
and to be able to discuss those in detail with your doctor.
How does hormone treatment help endometriosis?
Hormone treatment can be really effective at helping women
manage some of those symptoms of endometriosis.
And broadly, I think about hormone treatment
in two different ways.
There are contraceptives, like the oral contraceptive pill,
which contains oestregen and progesterone
and progesterone only pills like the mini pill,
and also progesterone only options like the implant,
the intrauterine system or the Mirena.
Those can all help by reducing the amounts
of endometrial tissue and alieving symptoms that way.
There are also other hormonal options which a
doctor might recommend.
These won't provide any contraceptive cover,
but will help to alleviate the symptoms of endometriosis.
It's really important that women remember
that there are loads of different options available
and each of these has benefits and also side effects.
So I'd really recommend
that people have a good front conversation
with their doctor or GP about what's going to work for you.
How does contraception help endometriosis?
Hormonal contraception can help to alleviate the symptoms
of endometriosis in a few different ways.
There are lots of different options for women.
People may have heard
of the combined oral contraceptive pill,
that contains oestrogen and progesterone,
and it works by stopping the ovaries from releasing an egg
from ovulating each month,
and it also can thicken the cervical mucus.
Because you're not ovulating, it can help relieve some
of those monthly symptoms of endometriosis.
There are also lots
of progesterone only contraceptives available.
Progesterone is important
because the contraceptives act to thin the lining
of the womb, and that helps to relieve particularly some
of the bleeding and pain related symptoms of endometriosis.
Options there include the progesterone only pill,
you might have heard that, called the mini pill.
Also, the intrauterine system, may have heard
that, called the marina or the injection or even the implant.
Those are all progesterone only options.
It's really worth talking to your doctor about
what you think is going to work best for you
and what the benefits versus the side effects are so
that you can make the best decision for yourself.
How does surgery help endometriosis?
One of the complications of endometriosis is
that the endometrial tissue that normally lines the womb
can sometimes occur outside the womb
in places like the ovaries, the fallopian tubes,
and even in other areas of the pelvis,
or areas like the bladder
or bowel. Surgery is an option to be able
to remove some of that tissue
and the kind of surgery that you are going
to be recommended will really depend on lots
of different factors, including
how severe the endometriosis is and where it is.
So it's really worth speaking to your doctor about that.
What happens during a surgery for endometriosis?
In endometriosis, the lining of the womb
or the endometrium can grow outside the womb.
So in places like the ovaries, the fallopian tubes, areas
around the pelvis, and even in areas like the bladder
or the bowel. The aim of surgery is to remove these areas
to be able to help to alleviate symptoms
for people suffering from endometriosis.
Now, the kind of surgery
that you'll be recommended depends on lots of things.
It will depend on where the endometriosis is
and how bad it is, but also on patient preference.
And two words that you might hear are laparoscopy
and hysterectomy.
Laparoscopy is the most common of those two,
and it's an operation that's done under general anaesthetic,
so you'll be asleep, and it's where
a few small cuts are made in the tummy,
and one is made in your belly button
where a camera is inserted,
and that allows the surgeon to be able to look
around the pelvis and see any areas of endometriosis
and to be able to remove them.
Recovery is really quick from that.
A hysterectomy is used more rarely,
and that's a much bigger operation, so that's
where the womb is removed, either through
a larger cut in the tummy or through the vagina.
It takes quite a long time to recover from, and of course,
because the womb is removed, there's no going back in terms
of planning, pregnancy, et cetera.
It's also also worth remembering that endometriosis
outside the womb can reoccur afterwards.
For that reason, it's really worth having a really in-depth
discussion with your doctor around
what the risks versus the benefits of these kinds
of operations are so
that you can make a really informed decision.
Will I need a hysterectomy to treat endometriosis?
Hysterectomy can be an option, tends to be an option
of last resort, for example,
after other treatments haven't worked so well and maybe
after women have had a laparoscopy or keyhole surgery to try
and remove some areas of endometriosis.
The reason why it tends to be a last resort
and not used as commonly is
because it's a really major operation.
It's done under general anaesthetic
and the womb is removed either
through a larger cut in the tummy or through the vagina.
It takes quite a long time to recover from,
and it's also only an option if you don't want
to get pregnant. For that reason,
you'll be really carefully counselled by the doctor around
what the options are in terms of a hysterectomy
and whether there might be any other treatment
options available to you.
That's important because it's valuable for you to be able
to balance what those risks of the treatment are versus
what impact the current symptoms are having on your life so
that you can make the best decision for yourself.
Will endometriosis get better on its own?
Everybody's endometriosis experience is different.
That means that without treatment, for some women,
the symptoms might get better by themselves,
but for some women, they may get worse.
That's why it's really important
to keep an eye on the symptoms over time.
That allows you to do two things:
it allows you to go and see your doctor
or GP if you've either seen a change in your symptoms
or if those symptoms are having a big impact on your life.
It also allows you
to make a judgement about when you might want
to start treatment and when you do,
or if you do, whether that treatment has been effective
for you.
Can I protect myself against endometriosis?
This is an area of current research.
At the moment, there is no indication
that endometriosis can be prevented,
but what is clear is that people
who are suffering from the symptoms of endometriosis
can reduce the impact of those symptoms,
but also potentially avoid any complications
of the endometriosis by being aware of those symptoms
and keeping a track of them by seeking a diagnosis as early
as possible, and by speaking really openly
with their doctor or GP around
what treatment options might be available to them so
that they can reduce any symptoms going forward.
How can I deal with pain during sex?
For people without a diagnosis of endometriosis, pain
during sex can be a warning sign, so it's really important
to go and speak to your GP or doctor about that.
Unfortunately, for people with a diagnosis of endometriosis,
pain during sex can be a symptom of the endometriosis.
Now, there are things that people can find helpful for that.
That can include taking some pain relief, changing position,
adding in some lubrication, and tracking your monthly cycles
because the pain might be worse at
certain points of the month.
However, if those things don't work
or if pain is so bad that you are not able to have sex
and it's affecting you
and your relationship, it's really important that you go
and speak to your GP or doctor about that
because there may be other issues
or treatments that are available for you.
Does endometriosis impact other organs or body functions?
The symptoms of endometriosis are really wide ranging
and it can include things like pain in the lower
pelvis or the back.
It can also affect your digestive system
and cause changes in your bowel habits in terms
of constipation or diarrhoea.
Obviously, all of these things can affect your mood
and we know that people can suffer from depression,
so it's really important
that if these symptoms are having an impact on your quality
of life, that you go and speak to your doctor
or GP who'll be there to support and help you.
Does endometriosis change as I get older?
Unfortunately, endometriosis appears
to be a lifelong condition.
It's an area of research,
but at the moment, there's no cure for endometriosis.
What is clear, however, is that people with endometriosis
who monitor their symptoms carefully
and start treatment if necessary, can really help
to alleviate some of those symptoms.
If you have any questions, it's really important to go
and speak to your doctor or GP in terms of
what the treatment options might be
and how they can support you better.
Can endometriosis lead to other conditions like cancer?
The effect of endometriosis
and its links to other conditions is an area
of ongoing research.
There is some evidence that it can be linked
to conditions like asthma and autoimmune conditions.
There's also some evidence that endometriosis,
whilst it doesn't cause cancer, can in some women
be associated with a higher risk
of developing ovarian breast or endometrial cancer.
But this is still an area of research.
It's really important that if you're concerned about any
of these areas that you speak to, your doctor
or GP who'll be able to advise you further.
Can endometriosis affect my mental health?
The symptoms of endometriosis are really wide ranging.
So for people with endometriosis who have painful
or heavy periods, who have other symptoms like abdominal,
pelvic, or back pain,
or even a challenge with issues like infertility,
that can really impact their quality of life.
All of those symptoms together can mean that people
with endometriosis can suffer from low mood or anxiety.
It's therefore really important to not just keep track
of your symptoms, but also it's impact on your
life and on your mood
and if you're struggling to be able to reach out
to a professional for help.
That's not necessarily just your GP or doctor.
There are lots of online support groups as well.
But if you feel that your mental health is struggling,
then we'd really recommend that you speak to a professional.
My endometriosis is affecting my quality of life, what should I do?
There are lots of things that people
with endometriosis can do in terms
of reaching out for more support.
I think a really good first port of call is
with your friends and family.
Let them know how you're feeling
and what impact it is having on your life.
I think a second place to look is lots of endometriosis
charities and online support groups might be able
to provide you with support that you might not be able
to necessarily get at home.
For some people, reaching out to their employer
to let them know how they're struggling might be helpful in
terms of making any adjustments to your work
to allow you to carry on.
Finally, if you're really struggling with the symptoms
of endometriosis,
and particularly if it's having an impact on your mental
health, it's really important that you speak
to your doctor or GP.
There are lots of different options available to you,
and it's really important
that people don't suffer in silence.
Do the endometrial cells that grow outside of the womb shed like in a normal period?
Normally the endometrial cells in the womb accumulate
and then they shed, and then that's what gives you a period.
In endometriosis.
Those endometrial cells can occur
outside the womb in areas like the ovaries
and the fallopian tubes in
and around the pelvis, for example.
Those don't shed like a period, so they won't cause a bleed,
but what they do do is they accumulate,
they can cause cysts, which can be really painful,
and they can also cause stickiness between different areas
of the pelvic organs, adhesions,
which can cause complications including increased pelvic
plane and may be associated with infertility as well.
It's therefore really important to keep track
of your symptoms because it might be an indication of some
of those complications of endometriosis,
which might be managed with treatments.
What is the difference between endometriosis & adenomyosis?
In endometriosis, the endometrial cells
that line the womb can grow
outside the womb in areas like the ovaries,
the fallopian tubes, areas around the pelvis,
and even in places like the bladder
or bowel. In adenomyosis,
in contrast, those cells can grow inside the muscular lining
of the womb and they still react like normal endometrial
cells in terms of breaking down and causing bleeding,
and they can put a lot of pressure on your bladder and bowel
because of that and cause painful and heavy periods.
It's therefore really important that if you have any
of those symptoms, you keep a close eye on them, understand
what impact it's having on your quality of life so
that you can speak to your GP
or doctor about any further tests that you might need
or treatment options that are available.
Does what I eat impact the symptoms of endometriosis?
There is some early research that shows
that dietary changes can improve the symptoms
of endometriosis, but there's no one size fits all solution.
Everybody's different.
So I'd recommend following a good, healthy, varied diet
and trying to maintain your weight.
Does exercise impact the symptoms of endometriosis?
There are some case studies that show that the symptoms
of endometriosis can be improved through regular exercise.
It's really important to keep a track of what symptoms
of endometriosis you are experiencing
and their impact on your quality of life.
That's because once you start exercising, whatever you do,
you'll be able to monitor what effect
that exercise is having on your physical and mental health.
What age am I most likely to be diagnosed endometriosis?
Endometriosis is a condition that can affect anybody
who's having menstrual cycles.
There's some evidence to suggest that it can take up
to 7.5 years for people with endometriosis to be diagnosed.
That means that most commonly it's people in their
later twenties, thirties,
and even up to their forties who are diagnosed.
However, it can also be diagnosed in people younger
and older than that.
Living with endometriosis? Looking for support?
The endometriosis support page in our Women's Health Hub offers a wide range of expert advice, information and tools.
The symptoms of endometriosis include pain in your pelvis, which is usually worse just before and during your period, and pain during or after sex. Other symptoms include heavy periods and feeling extremely tired. If you’re trying for a baby you might have some difficulty. But some people with endometriosis don’t get any symptoms.
For more information, see our section on symptoms of endometriosis.
If you get your symptoms under control with medicines or surgery, you should be able to live a normal life. Endometriosis can affect everyone differently. In some people, it gets progressively worse whereas in others it stays the same or even improves with time. It can lower your quality of life if the pain affects you at work and in your everyday life, so it’s important to get treatment.
There isn’t a cure so you can’t heal from endometriosis. Endometriosis symptoms often ease during pregnancy, and they may improve without any treatment. And it doesn’t always get worse with time – some studies have shown that endometriosis can reduce in up to a third of people studied.
The best way to treat endometriosis will depend on your individual circumstances. Your doctor will need to consider how bad your symptoms are, and if you want to have children in the future. Treatment options include different types of medicine and surgery. Your doctor will discuss the various options with you, and help you decide which endometriosis treatment is best for you.
For more information, see our section on treatment of endometriosis.
You can’t prevent endometriosis. Studies have looked at whether doing some regular exercise or taking the oral contraceptive pill may prevent endometriosis but didn’t find any proof. Doctors usually recommend a healthy lifestyle, which includes a healthy diet, not drinking too much alcohol and doing some regular physical activity.
Female infertility
Painful periods (dysmenorrhoea)
Gynaecological laparoscopy
In a gynaecological laparoscopy, your surgeon uses a camera (laparoscope) to see inside your lower abdomen (tummy). This means they will be able to see your womb (uterus), fallopian tubes and ovaries.
Hysterectomy
Heavy periods (menorrhagia)
Did our Endometriosis information help you?
We’d love to hear what you think. Our short survey takes just a few minutes to complete and helps us to keep improving our health information.
The health information on this page is intended for informational purposes only. We do not endorse any commercial products, or include Bupa's fees for treatments and/or services. For more information about prices visit: www.bupa.co.uk/health/payg
This information was published by Bupa's Health Content Team and is based on reputable sources of medical evidence. It has been reviewed by appropriate medical or clinical professionals and deemed accurate on the date of review. Photos are only for illustrative purposes and do not reflect every presentation of a condition.
Any information about a treatment or procedure is generic, and does not necessarily describe that treatment or procedure as delivered by Bupa or its associated providers.
The information contained on this page and in any third party websites referred to on this page is not intended nor implied to be a substitute for professional medical advice nor is it intended to be for medical diagnosis or treatment. Third party websites are not owned or controlled by Bupa and any individual may be able to access and post messages on them. Bupa is not responsible for the content or availability of these third party websites. We do not accept advertising on this page.
Reviewed by Rachael Mayfield-Blake, Freelance Health Editor, January 2023
Expert reviewer, Dr Madhavi Vellayan, Consultant Gynaecologist
Next review due January 2026
- Endometriosis patient information leaflet. Royal College of Obstetricians and Gynaecologists. www.rcog.org.uk, published December 2023
- Endometriosis: diagnosis and management. National Institute for Health and Care Excellence (NICE). www.nice.org.uk, last updated 11 November 2024
- Endometriosis. NICE Clinical Knowledge Summaries. cks.nice.org.uk, last revised November 2024
- Information on endometriosis. European Society of Human Reproduction and Embryology (ESHRE). www.eshre.eu, reviewed 2022
- Endometriosis. Medscape. emedicine.medscape.com, updated 18 July 2023
- Endometriosis. BMJ Best Practice. bestpractice.bmj.com, last reviewed 27 February 2025
- Endometriosis. Patient. patient.info, last updated 18 February 2025
- What is endometriosis? Endometriosis UK. www.endometriosis-uk.org, last reviewed November 2024
- Genital examination in women. Royal College of Nursing. www.rcn.org.uk, last updated 6 November 2023